Employees Retirement System of Texas PO. The enrollment form must be received at the GIC within 60 days of the return to work.
Http Www Rdgins Com Active Webdoc Asp S 396976512 P 546431360
Equipment Your Choice HOW TO APPLY FOR COVERAGE For Fastest Service.

Insurance enrollment form. Single Divorced Married Maiden Name _____. If you have questions about your information or believe that. International Health Insurance Enrollment Form Enroll in international health insurance offered through SUNY as an international scholar OPT or facultystaff member.
If you did not yet read the informational insurance information please do that before completing and submitting this form. This enrollment form can be quickly shared anywhere online with just a copy-paste. Please send this completed form to.
Box 13207 Austin Texas 78711-3207. General Liability 2000000 PART 3. Accident Insurance Enrollment Form - California.
And such documents aim to gather the applicants details for recordkeeping. I designate the following persons as primary beneficiaryies for any amount payable upon my death for the Lincoln Financial Group insurance coverage applied for in this Enrollment Form. SILA HEALTHCARE ENROLLMENT FORM 2021.
And your respondents will be able to fill in the form from any device. Health Benefits Election Form Form Approved. And to process the registration enrollees fill in the blanks of a form specifically the enrollment form.
By submitting this Enrollment Form I am aware that for assignment of benefit claims the specialty pharmacy may ship product upon verification of benefits and collection of applicable co-pay. All information shared on this form is secure and private. Crime 25000 PART 5.
Hence enrollment forms are the official documents used to apply for programs and services of choice. Accident Insurance Enrollment Form - New Hampshire. Or Suspend your FEHB enrollment.
Group Number 753781. Last Name First Name Middle Name Address. Life Health Marital Status.
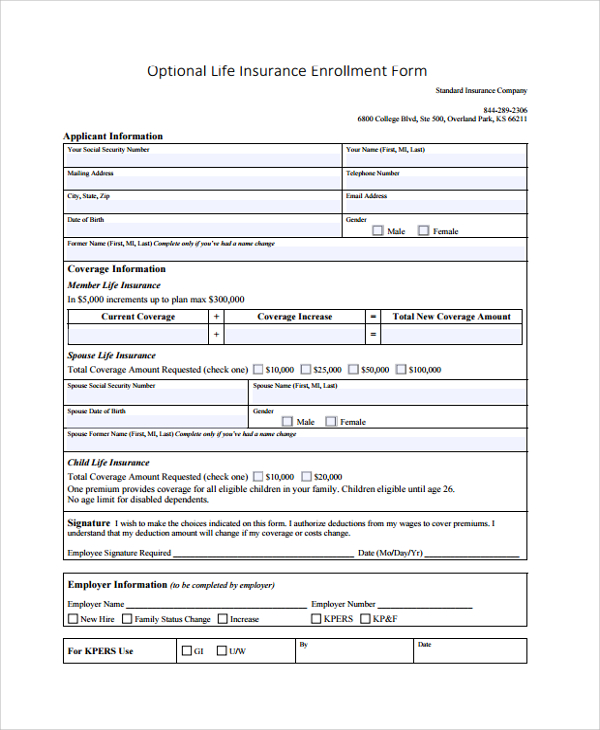
For those that previously received their Form 1095-B in the mail you can receive a copy of your Form 1095-B by going out to the Aetna Member Website in the Message Center under the Letters and Communications tab or by sending us a request at Aetna PO BOX 981206 El Paso TX 79998-1206. D-753781 SI 7533 Page 1 of 1 1019 Optional Life Insurance Enrollment Form. GROUP INSURANCE ENROLLMENT FORM Group Policy No.
Uses for Standard Form SF 2809 Use this form to. We will continue to provide the 1095-B form to members who live in the. 2021 INSURANCE PLAN ENROLLMENT FORMS COVERAGES LIMITS AVAILABLE PART 1.
RETIREE INSURANCE ENROLLMENT FORM. With such designation any previous designation of a beneficiary for such coverage is. Or Enroll or reenroll in the FEHB Program.
Or Elect not to enroll in the FEHB Program employees onlyor Change your FEHB enrollment. Are returning from a military leave. Supersede enrollment You have 30 days following your employment date to make any additions or changes to the coverage you elected.
Online Insurance Enrollment Form Directions for Successful Completion and Submittal 1 If you are currently enrolled in any one or more insurances you can find your current deductions and coverage level at the top of the PEF MBP home page under My Deductions. Information provided to ERS may be incorrect please notify ERS. Information provided to ERS is maintained for managing your.
Date of Hire. Accident Medical Expense 250000 PART 2. Or Cancel your FEHB enrollment.
- Month - Day Year. Click here if you are filling out this form because you are a new employee. Qualifying Life Event.
Many translated example sentences containing insurance enrollment form French-English dictionary and search engine for French translations. Accident Insurance Enrollment Form. Fax completed form to The Standard at 971-321-5033 or mail to address above.
Accident Insurance Enrollment Form - New Jersey. Collect manage data. Such form with this Enrollment Form in a manner and on a form consistent with the requirements in my state.
Health Insurance Enrollment Form Complete the Enrollment Form to Elect or Decline Coverage Complete the Enrollment Form for the New Hire Process Elect or Decline Medical Coverage on the Enrollment Form You MUST Sign and Date the Bottom of the Form even if you Decline Coverage Return the Enrollment Form to your Branch Manager. I understand that if there is no co-pay the patient may not be. Day I Month I Year Coverage.
Work Hours and Eligibility Active state employees must work at least 1875 hours in a 375-hour workweek or 20 hours in a 40-hour workweek. Accident Insurance Enrollment Form - Louisiana. Directors Officers Liability 1000000 PART 4.
You must make your elections and sign the Insurance Enrollment Form or Insurance Change Form within 30 days of the qualifying event the date the loss occurred. Forms received after 60 days are returned and you may re-apply during Annual Enrollment. In order to make changes you must submit a new Insurance Enrollment Form.
Switch designated eligible family member. Accident Insurance Enrollment Form - Florida. Embed it in a websites code or as a popup lightbox on a social media page or send the form URL to an email list if that option suits you better.
Standard Insurance Company 844-289-2306.
Fillable Online Aetna Health Insurance Enrollment Form Engineering Resource Fax Email Print Pdffiller
 Free 8 Sample Enrollment Forms In Pdf Ms Word
Free 8 Sample Enrollment Forms In Pdf Ms Word
Http Kurz Com Wp Content Uploads 2014 09 Health Enrollment Pdf
 Health Insurance Enrollment Change Form Manualzz
Health Insurance Enrollment Change Form Manualzz
 10 Insurance Application Forms Pdf Free Premium Templates
10 Insurance Application Forms Pdf Free Premium Templates
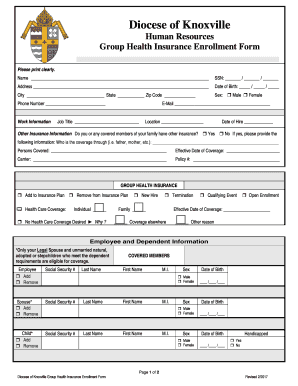 Fillable Online Group Health Insurance Enrollment Form Fax Email Print Pdffiller
Fillable Online Group Health Insurance Enrollment Form Fax Email Print Pdffiller
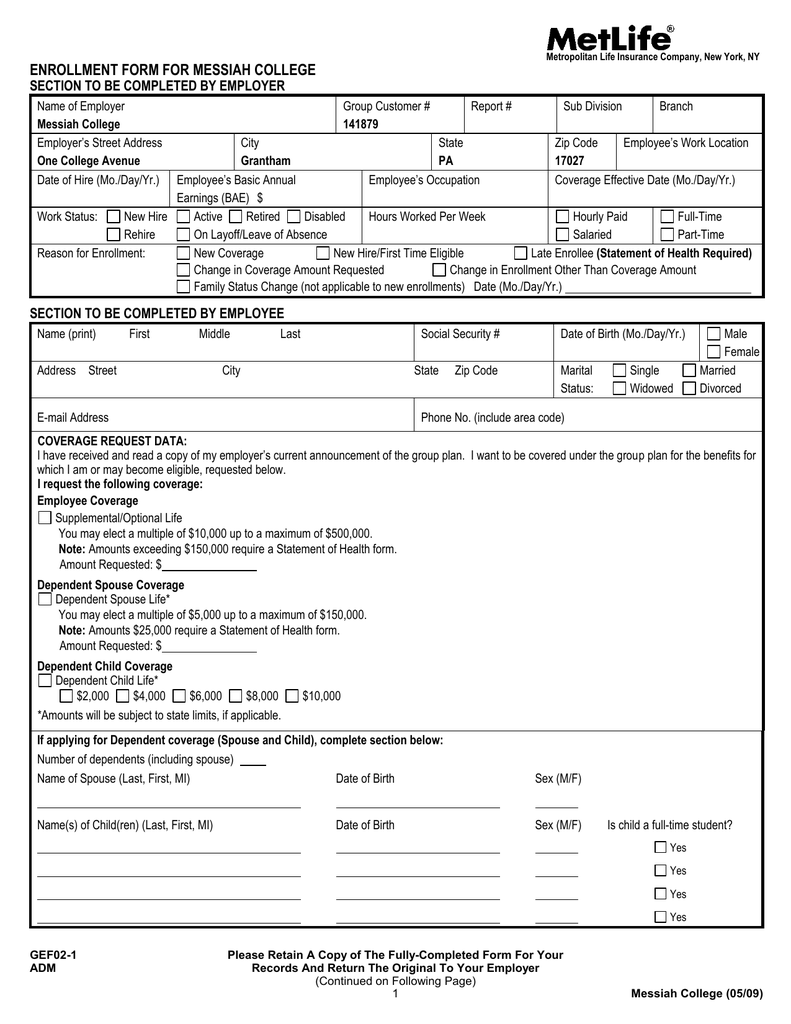 Metlife Voluntary Life Enrollment Form
Metlife Voluntary Life Enrollment Form

 Southland National Voluntary Plan Enrollment Form Lg07
Southland National Voluntary Plan Enrollment Form Lg07
 Fillable Online Group Insurance Enrollment Form Barp Fax Email Print Pdffiller
Fillable Online Group Insurance Enrollment Form Barp Fax Email Print Pdffiller
 Fillable Online Beh 10 Health Insurance Enrollment Form Fax Email Print Pdffiller
Fillable Online Beh 10 Health Insurance Enrollment Form Fax Email Print Pdffiller
Https Portal Rfsuny Org Portal Page Portal Employee Benefits Files Benefits Enroll Form Pdf
 Fillable Online Ccri Health Insurance Enrollment Form Community College Of Rhode Ccri Fax Email Print Pdffiller
Fillable Online Ccri Health Insurance Enrollment Form Community College Of Rhode Ccri Fax Email Print Pdffiller
 Employee Enrollment Form Park Avenue Insurance
Employee Enrollment Form Park Avenue Insurance



No comments:
Post a Comment
Note: Only a member of this blog may post a comment.