Before you dive in to Part I write your name and Social Security number at the top of the form. Filling out Form 8962 and finding an example of Form 8962 filled out can feel stressful.
 Premium Tax Credit Form 8962 And Instructions
Premium Tax Credit Form 8962 And Instructions
Form 8962 is used either 1 to reconcile a premium tax credit advanced payment toward the cost of a health insurance premium or 2 to.
Where do i get form 8962. Part I is where you record annual and monthly. To enter your 1095-A form and generate an 8962 form. The IRS will provide more details on IRSgov.
DRAFT AS OF July 24 2014 DO NOT FILE Early releases of draft forms and instructions are at IRSgovdraftforms. The IRS fax number for 8962 form is 1-855-204-5020. Quick steps to complete and e-sign Form 8962 online.
To speed the process try out online blanks in PDF. Get And Sign Irs Fax Number For 8962 Form Generally are subject to OMB approval before they can be officially released. Open the doc and select the page that needs to be signed.
Start completing the fillable fields and carefully type in required information. Click on View or Print Forms to print the forms you need. Print save or preview this years return and click in the box to select federal returns.
The form may be available in packages of print forms. Follow these steps carefully and prepare for this years taxes. It is used to report your credit amount on your tax return and reconcile the advance credit payments made on your behalf.
Taxpayers in this situation should not file an amended return solely to get a refund of this amount. Click Done with Health. Name shown on your return.
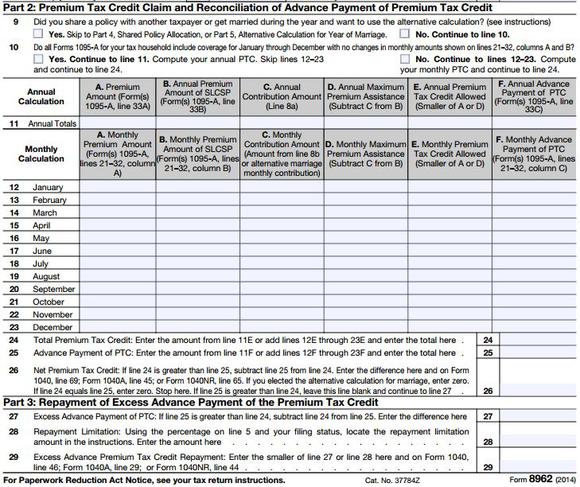
Organizing your documents and carefully going through the forms ensures you receive the returns you need and deserve. Form 8962 Department of the Treasury Internal Revenue Service Premium Tax Credit PTC Attach to Form 1040 1040-SR or 1040-NR. Use the Cross or Check marks in the top toolbar to select your answers in.
An individual needs 8962 Form to claim the Premium Tax Credit. Get form 8962 2018 signed right from your smartphone using these six tips. Form 8962 is available on the IRS website.
If you dont have an account yet register. Your social security number. IRS Form 8962 A premium tax credit or PTC is a type of refundable tax credit that allows low income and middle income individuals and families cover the premiums of health insurance bought in the Health Insurance Marketplace.
3 Form 8962 is a two-page form broken into five parts. If youre mailing in a paper tax return and you received advance payments of your health insurance premium tax credit youll need to file a completed Form 8962 with your regular tax return forms. Again IRS is taking steps to reimburse people who filed Form 8962 reported and paid an excess advance Premium Tax Credit repayment amount with their 2020 tax return before the recent legislative changes were made.
You can apply digital IRS form 8962 to learn your PTC amount. You can get the IRS Form 8962 from the website of Department of the Treasury Internal Revenue Service or you can simply download IRS Form 8962 here. Drafts of instructions and publications usually have at least some changes before being officially released.
Part I is where you enter your annual and monthly contribution amounts. August 27 2020 How to. Form 8962 is divided into five parts.
Youll enter the number of exemptions and the modified adjusted gross income MAGI from your 1040 or 1040NR. Download the form and open it using PDFelement and start filling it. Steps to Fill out Online 8962 IRS Form.
Use Get Form or simply click on the template preview to open it in the editor. Select Tax Tools on the left menu. Search for the document you need to e-signelectronically sign on your device and upload it.
The 8962 form will be e-filed along with your completed tax return to the IRS. Its only required to fill empty fields. On the Thats all we need on your 2017 coverage screen 10.
Information about Form 8962 Premium Tax Credit including recent updates related forms and instructions on how to file. Go to wwwirsgovForm8962 for instructions and the latest information. If you did not e-file your return with the Form 8962 for the Premium Tax Credit the IRS might send you a letter asking for this information.
If you filled out the form during one of the previous years itll make an example of form 8962 filled out.